Blog
The Invisible Third of Your Life

There is a third of your life you don’t experience. You sleep through it. You don’t remember most of it. But your body is doing some of its most important work in those hours — clearing metabolic waste, consolidating memory, repairing tissue, recalibrating hormones for the day ahead. For people without diabetes, this happens quietly. For people with diabetes, the same biological machinery that maintains everyone else’s overnight glucose has to be approximated by hand, by hardware, or simply hoped through.
It helps to start with what’s actually happening in there.
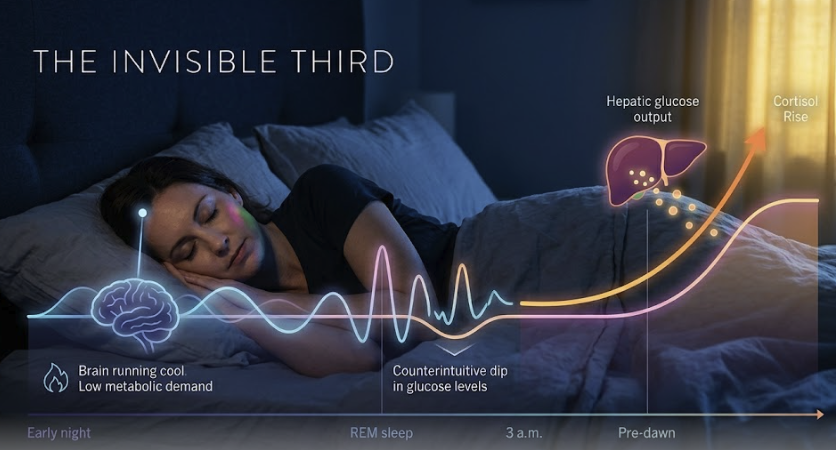
Around 3 a.m., the body begins preparing to wake. Cortisol begins its pre-dawn climb. Growth hormone, which was released in pulses during the deep slow-wave sleep of the first half of the night, has already done its work suppressing insulin sensitivity. The liver, reading these signals, starts releasing glucose into the bloodstream — endogenous glucose production, ramping up to fuel the morning. In someone without diabetes, the pancreas matches this rise with a quiet, perfectly timed bump of insulin. Glucose stays flat. Nobody notices. The day begins.
In diabetes, that match doesn’t happen. The signal is the same. The response isn’t. Roughly half of people with type 1 diabetes and a similar fraction of people with type 2 experience a measurable dawn rise driven by this growth-hormone-mediated cascade between 3 and 8 a.m. (Porcellati et al., Diabetes Care, 2013). Monnier’s earlier work pegged the prevalence in type 2 at around 55%. Pearson’s 2020 paper in JCEM mapped the cortisol arc more precisely — a steady nocturnal climb that drives hepatic glucose output well before the alarm clock goes off. None of this is a failure of effort. It is endocrinology doing exactly what it evolved to do, in a body that can no longer answer for itself.
Then there is the other half of the night.
Sleep is not a single state. It cycles. Slow-wave sleep dominates the early hours; REM dominates the later ones. These are biochemically different countries. In slow-wave sleep, the brain runs cool and metabolic demand is low. In REM, neuronal activity spikes to near-waking levels, and so does the brain’s appetite for glucose. The result is a counterintuitive piece of physiology that almost nobody talks about: REM is the high-risk window for hypoglycemia. Pillai and colleagues, working with continuous glucose data across sleep stages, found hypoglycemia occurred at roughly 5.5% of REM epochs versus 0.5% of deep-sleep epochs (J Diab Sci Tech, 2013). Eleven times more often in the stage of sleep most people associate with vivid dreaming, not danger.
That number lands harder when you put it next to two others. Kulzer’s 2024 review documented that more than half of severe hypoglycemic events happen during sleep, and that hypoglycemia awareness — the body’s ability to self-rescue with adrenaline and a pounding heart — is attenuated during REM. The system that would normally wake you doesn’t. Cappon’s 2024 work added another layer: people who hit their daytime Time-in-Range targets are not necessarily nocturnally safe. Overnight events are longer, deeper, and more often unrecognized than their daytime counterparts. A “good” CGM report can hide a bad night.
There is one more thread worth pulling, because it touches everyone, not just people with diabetes. In 2010, Donga and colleagues took healthy adults — no diabetes, no metabolic disease — and restricted them to a single four-hour night. The next morning, they were measurably insulin-resistant (JCEM, 2010). One short night. In a healthy body. The takeaway isn’t that sleep loss causes diabetes. It’s that sleep is not a passive state where metabolism waits for morning. Sleep is metabolism. Disturb it and the next day’s glucose tells on you.
Put it all together and the picture is this: the overnight hours are the part of the day where the most glucose-relevant biology happens, the part where the patient has the least ability to intervene, and the part where the consequences of getting it wrong are largest and least visible. The dawn rise is real. The REM dip is real. The cortisol arc is real. The liver does not pause for the patient’s convenience. And the alarm-bell physiology that should wake someone falling low gets quieter in the very stage of sleep when the risk is highest.
People who live with diabetes already know all of this without the citations. They know it as the 3 a.m. taste of glucose tablets, the morning number that doesn’t match the bedtime number, the day after a bad night when nothing tracks right. The science just names what the body has been telling them.
The point of writing it down is not to alarm anyone. The body’s overnight work is, on balance, miraculous — a coordinated handoff between brain, liver, adrenals, and pituitary that runs every night for a lifetime. The point is that when one piece of that handoff is missing — the pancreatic beta cell, doing its quiet matching work — the rest of the system keeps running on its original program. That program assumes a partner that isn’t there.
Sleep-only automation exists because that partner can be supplied where it’s needed most: in the third of life nobody is awake to manage.
Nights protected. Days yours.
Research Sources
Topic 1 — Dawn Phenomenon
Monnier L, et al. “Magnitude of the Dawn Phenomenon and Its Impact on the Overall Glucose Exposure in Type 2 Diabetes.” Diabetes Care, 2013. — Dawn phenomenon present in ~55% of T2D patients (n=248); average pre-dawn-to-post-dawn glucose rise ~16 mg/dL. Landmark. [Pre-2015, seminal]
Porcellati F, et al. “Thirty Years of Research on the Dawn Phenomenon.” Diabetes Care, 2013;36(12):3860. — ~54% T1D and ~55% T2D exhibit dawn phenomenon. Mechanism: GH-mediated reduction in hepatic/peripheral insulin sensitivity 3am–8am. [Pre-2015, seminal]
StatPearls. “Dawn Phenomenon.” NCBI NBK430893 (continuously updated). — In diabetes, the pre-dawn compensatory insulin mechanism fails, producing fasting hyperglycemia. NIH-curated.
Topic 2 — Cortisol and Growth Hormone
Pearson MM, et al. “Novel Insights Into Effects of Cortisol and Glucagon on Nocturnal Glucose Production in T2D.” J Clin Endocrinol Metab, 2020. PMC7274493. — Rising nocturnal cortisol drives increased endogenous glucose production overnight in both T1D and T2D. High methodologic rigor (tracer study).
Søfteland E, et al. “Cortisol as a Predictor of Nocturnal Hypoglycemia.” PMC12417556, 2024. — Lower evening cortisol significantly associated with increased nocturnal hypoglycemia risk. Cross-sectional; needs replication.
Topic 3 — Sleep Stages and Glucose Variability
Pillai A, et al. “Nocturnal CGM and Sleep Stage Data in Adults with T1D.” J Diabetes Sci Technol, 2013. PMC3876379. — Hypoglycemia rate: 5.5% during REM vs. 0.5% during deep sleep. BLOG NOTE: REM is the high-risk window, not deep sleep. [Pre-2015]
Brandt R, et al. “Sleep Quality and Glycaemic Variability in T1D.” Diabetologia, 2022. PMC9254230. — Poor sleep quality significantly associated with greater overnight glycemic variability.
Topic 4 — Nocturnal Hypoglycemia in MDI
Kulzer B, et al. “Nocturnal Hypoglycemia in the Era of CGM.” J Diabetes Sci Technol, 2024. — >50% of severe hypoglycemic episodes occur during sleep. Awareness is attenuated overnight; repeated events induce IAH. Expert review.
Cappon G, et al. “Characteristics of Nocturnal Hypoglycaemic Events.” PMC11418509, 2024. — Nocturnal events common in T1D MDI even when TIR targets are met; longer in duration, more often unrecognized. KEY POINT: TIR-on-target ≠ nocturnally safe.
McAuley SA, et al. “Nocturnal Hypoglycemia: Pumps vs. MDI.” Diabetes Technol Ther, 2020. — At equivalent TIR, MDI users experience more nocturnal hypoglycemia than pump users.
Topic 5 — Sleep Deprivation and Insulin Resistance
Donga E, et al. “A Single Night of Partial Sleep Deprivation Induces Insulin Resistance.” J Clin Endocrinol Metab, 2010. PMID 20371664. — One night of 4-hour sleep produced measurable insulin resistance in healthy adults (clamp). [Pre-2015, landmark]
Systematic review (PMC9036496), 2022. — Majority of included studies show glucose tolerance and/or insulin sensitivity substantially impaired when sleep restricted for days to weeks.



